Its not. The x-rays should have been the key to solving the JFK assassination (whether he was shot from the front or back) but instead they tell us JFK was shot with a 6.5mm semi-circular blob that Dr. Mantik has become obsessed about.
I agree that the medical evidence (the autopsy report, the X-rays, the photographs) in any murder case is of the utmost importance, but in the assassination of the President it has been tainted by stories of destroyed autopsy evidence, missing autopsy evidence, multiple original autopsy reports, altered photographs and X-rays, conflicting witness statements about the location and size of the wounds and so on.
Take the head wound. At autopsy it was determined that the bullet had entered the back of JFK's head LOW, a little above and to the right of the EOP, and created a large exit wound in the parietal bone, extending into the temporal and occipital regions.
The HSCA relocated the entry wound in the skull to the top of the head, while limiting the large exit wound almost entirely to the parietal region - at least that is how it appears in the Dox drawing.
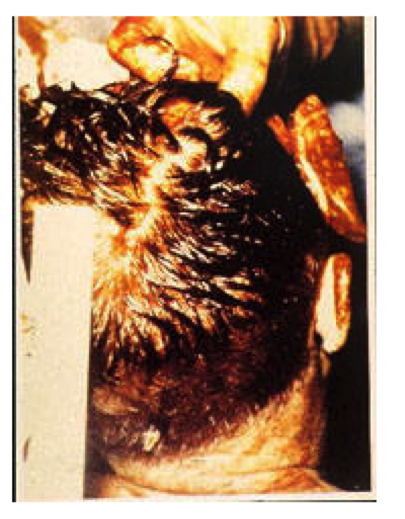
The autopsy photograph of the back and top of the head does not show any of these wounds, except the bone flap which is in the back of the photo. The purpose of the picture is unclear, and the reason the ruler is held near the head and what exactly it is measuring is anybody's guess, as it can't be there to measure the size of the bullet hole in the cowlick, as the pathologists had located the entry wound 4 inches lower.