First, where does Gregory say that a fragment had penetrated into the femur? It's not in his operative report. In his WC testimony, he describes it as "a fragment of metal, again microscopic measuring about five-tenths of a millimeter by 2 millimeters, lies just beneath the skin, about a half inch on the medial aspect of the thigh." "Just beneath the skin" just doesn't quite generate that embedded-in-the-femur vibe.
You are right that Gregory did not go quite as far as Shires and did not say that the fragment was in the femur. But Gregory did say that xrays showed that a fragment was lying close to the femur (6H99):
"Mr. SPECTER. What did the X-rays reveal with respect to the presence of a missile?
Dr. GREGORY. In the thigh there was a very small shadow, perhaps 1 mm. by 2 mm. in dimension, lying close to the medial aspect of the femur, that is, the thigh bone, but was in my opinion much too small to have accounted for the dimensions of the wound on the medial aspect of his thigh or a wound of that character."
Shires said that the fragment was in the femur (6H106):
"Dr. SHIRES. The wound on the thigh was a peculiar one. There was a 1 cm. punctate missile wound over the junction of the middle and lower third of the leg and the medial aspect of the thigh. The peculiarity came in that the X-rays of the left leg showed only a very small 1 mm. bullet fragment imbedded in the femur of the left leg. Upon exploration of this wound, the other peculiarity was that there was very little soft tissue damage, less than one would expect from an entrance wound of a centimeter in diameter, which was seen on the skin. So, it appeared, therefore, that the skin wound was either a tangential wound or that a larger fragment had penetrated or stopped in the skin and had subsequently fallen out of the entrance wound."
In Shires' medical report he says (CE392, 17H535) :
"X-rays of the thigh and leg revealed a bullet fragment which was imbedded in the body of the femur in the distal third."
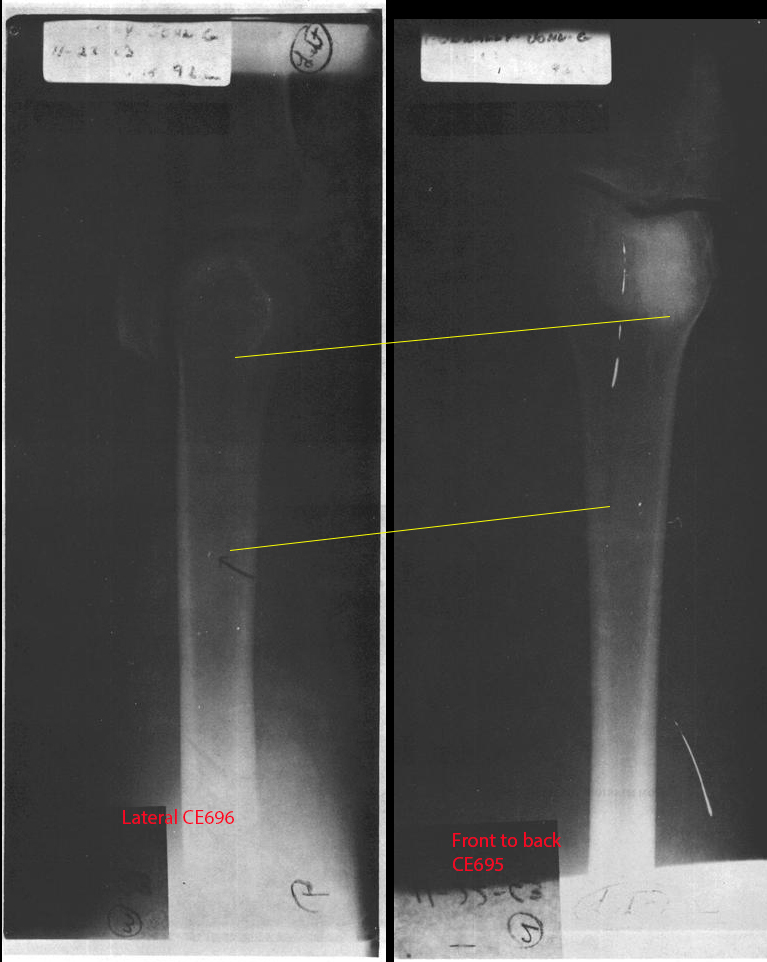
They were looking at these same xrays, presumably:
Those xrays are certainly consistent with the fragment being embedded in the femur and the condition of CE399 indicates that the butt end struck something hard enough to dent it. It is consistent with some kind of sudden impact causing the bullet to dent and to shed a fragment. Dr. Shires explored the bullet tract down to the region of the femur and did not find the fragment in the tissue.
Second, the HSCA interviewed Dr Jack Reynolds, the Parkland diagnostic radiologist responsible for examining the x-rays in the days after the shooting. Reynolds also placed the fragment near the surface: "the location of this fragment as just beneath the skin in the region of the subcutaneous fat" and "the fragment is definitely not imbedded in the femur." The HSCA also asked Shaw for his opinion. Shaw "could not detect any metal fragments in the chest or in the femur," but he put a fragment "in the subcutaneous tissue in the thigh." They also ran Connally's x-rays past their own independent radiology consultants. One, Dr William Seaman put the fragment just beneath the skin and noted "there is no metal fragment in the femur." The members of the HSCA Forensic Pathology Panel, after reviewing the x-rays themselves, agreed with Reynolds, Gregory, Seaman, and Shaw. This is one issue where Dr Shires is in a very, very small minority.
The Connally x-rays contain a number of bright "artifacts" within the images that could be mistaken for an metal fragment. the HSCA report suggests that Shires mistook one of these to be an image of the bullet fragment within the femur.
Perhaps you can explain how an "artifact" or defect in the film can occur at different locations on two films and yet at the exact same location relative to the bone. The top yellow line in the above photo is between the same points of the bone. The lower yellow line is between the two marks that were identified as the fragment. They are at the same location in the bone.
I find it hard to believe that a bullet could strike Connally's femur hard enough to force a metal fragment deep into the bone without generating fractures and other significant damage that would easily show on the x-rays.
No one is saying it is
deep into the bone. The xrays don't show that much information. They really only show that it is very close to the bone and consistent with it being embedded on the surface of the bone. But why would it be hard to believe that the butt end of the bullet struck the femur and left a lead fragment? Lead is relatively soft as a metal. The butt end struck something - enough to dent it.
So, am I correct in understanding then that
if Shires was correct, you don't disagree that the thigh wound could have been made by a separate bullet?


